

 Doniraj
Doniraj
Therapy
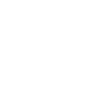
The treatment of MS has changed dramatically in last twenty years. From a disease for which there was no medicine, we came to 14 registered original medicines. The greatest advancement in neurology is related to the treatment of MS and this relapse-remittent form of MS (RRMS). Picture 1
Slika 1. Development of multiple sclerosis therapy in last 20 years, the original display of available drugs
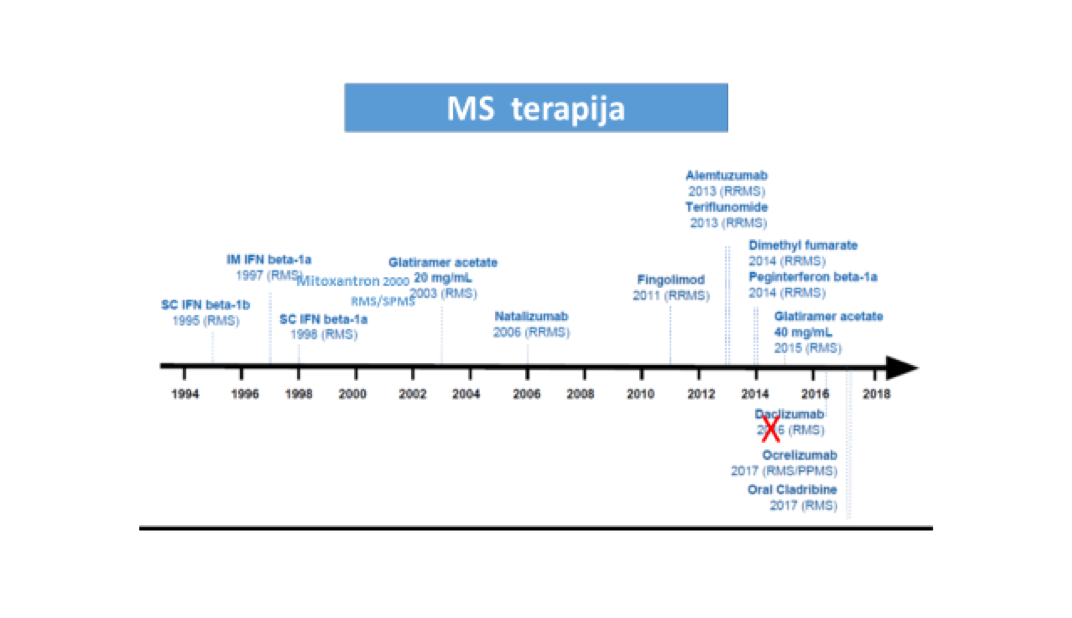
The basic postulate of MS treatment is that the therapy must start as early as possible i.e. immediately after the diagnosis of MS. Delaying the therapy means accumulation of damage and rapid attainment of severe neurological and functional deficits. It is well known from the study of monitoring the natural course of the disease, that MS patients who have not received any treatment, that after 20 years of the disease 50% of untreated patients MS are walking with help of a cane, and that, after 30 years of 70% of them are in a wheelchair. Patients who receive treatment from the very beginning of the disease, have a completely different course and reach significantly lower neurological deficit that is reflected in their functionality – they finish school, stay employed, raise families, remain active members of society with personal, family and professional affirmation. The importance of early therapy is best shown in in Picture 2.
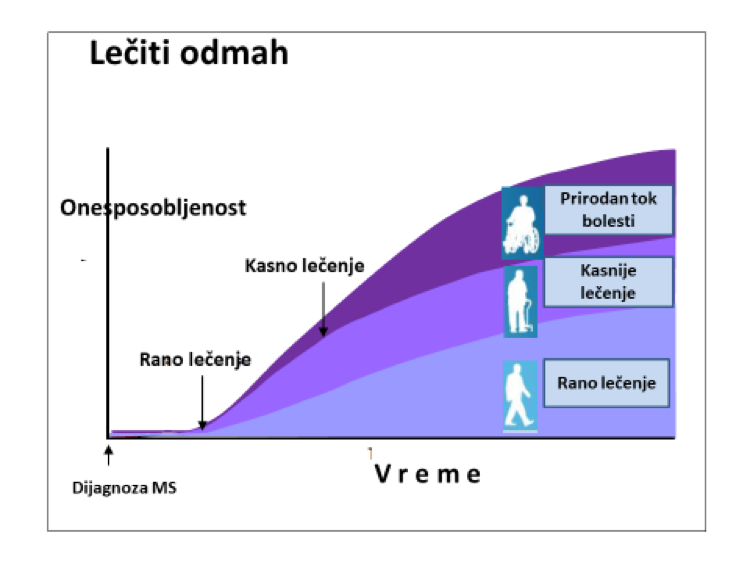
The first registered drugs belong to a group of immunomodulatory drugs i.e. drugs that modulate the pathological immune response present in the MS. They achieve this, simply said, by influencing various immune mechanisms, by inhibiting those that contribute to inflammation and damage, and by promoting those who have anti-inflammatory effect. Over the last two decades, these drugs have shown their efficacy in reducing relapse count, reducing the number of new lesions at MRI brain imaging and to a certain extent, slowing down the progression of neurological disability. Also, they’ve proved to be very safe drugs without causing significant unwanted effects. This group includes first-generation drugs: interferons – Interferon beta 1 (Rebif and Avonex), Interferon beta 1b (Betaferon) and glatiramer (Copaxone). All of these drugs require continuous use in order to maintain their therapeutic effect and be administered by injecting (subcutaneously or intramuscularly). After these drugs, new drugs develop and emerge, more effective than the first group of medications. This was necessary, because it was shown that huge number of patients couldn’t maintain disease under control with first generation drugs. Second generation drugs are by their nature and effect, immunosuppressive, thus acting on the inhibition of pathological immune responses with the aim of suppressing it and preventing further central nervous system (CNS) damage. So now we have monoclonal antibodies: natalizumab (Tysabri), alemtuzumab (Lemtrada) and ocrelizumab (Ocrevus), as well as oral immunosuppressive therapy: cladribine (Mavenclad), fingolimod (Gylenia), teriflunomide (Aubagio) and dimethyl (Tecfidera). There is another one too, highly effective immunosuppressant drug, mitoxantrone, which has been significantly less used for the past years due to fear of harmful side effects (cardiotoxicity and AML risk). Listed drugs have different efficacy, different safety profile and require different modalities of monitoring adverse effects. Graph 1 shows their efficiency related to NEDA criteria (results from registration studies). NEDA is new criteria for evaluation the effectiveness of MS therapy. NEDA means – No Evidence of Disease Activity, meaning no signs of disease activity! It is very strict and therefore very good criteria, because it measures three essential factors for disease control. First one is the absence of new relapse / worsening of the disease, while patients are on therapy. The second one is the absence of new lesions / damage to MRI examinations of the brain and spinal cord, and the third one is the absence of further progression of the disease, i.e. further worsening in neurological status. Achieving NEDA criteria, we can say with certainty that the disease is under control and that the therapy is effective.
Graph 1. Results of the efficacy from various drugs while respecting the NEDA criteria (results are from the registration studies of these drugs, source: Gavin Giovannoni SlideShare)
If the first postulate of treatment is to initiate therapy as early as possible, the second postulate is individual treatment approach. This means that the therapy is chosen according to the patient, the characteristics of his disease and the activity of the MS. Decision on the choice of therapy should be made by a neurologist, more precisely a MS neurologist, respecting these principles and consulting with the patient. It is very important that the patient understands what can be achieved and with what kin d of therapy can be achieved i.e. how effective it is, and whether there are and what are the risks of treatment.
About the choice of therapy in next post on our site.
Prof. Dr Dragana Obradović





